
Every three minutes, someone in the United States is diagnosed with cancer. For most cancers, the story of the past decade has been one of remarkable progress: new drugs, longer lives, and in some cases, cures where none existed before. For one cancer, however, that story has barely changed.
In 2026, an estimated 67,530 Americans will be diagnosed with pancreatic cancer, and 52,740 are expected to die from the disease. Pancreatic cancer remains the only major cancer with a five-year survival rate below 20% (currently stalled at 13%) and the third-leading cause of cancer-related deaths in the United States, behind only lung and colorectal cancers.
What makes this particularly painful is the context. Immunotherapy (a class of drugs that harnesses the body’s own immune system to fight cancer) has transformed outcomes for patients with melanoma, lung cancer, and bladder cancer. Five-year survival rates in some melanoma subgroups have climbed above 50%. Yet in pancreatic cancer, these same drugs have produced almost no meaningful benefit for the vast majority of patients.
This is the immunotherapy gap. Understanding why it exists, and whether it is finally beginning to close, matters enormously for the tens of thousands of patients diagnosed every year.
A Disease That Has Refused to Yield
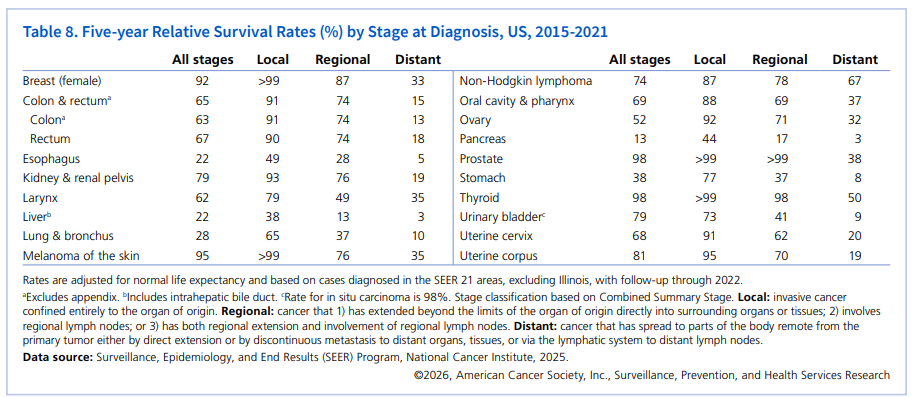
2026″, American Cancer Society
The numbers are stark. The five-year survival rate for pancreatic cancer has stalled at 13% for the third year in a row, according to Cancer Statistics 2026 from the American Cancer Society. For those diagnosed with pancreatic adenocarcinoma (the most common form of the disease) that figure drops to just 8%.
The late-diagnosis problem compounds everything. Surgery with pancreatectomy offers the only chance of a cure, but only about 15 to 20% of patients are eligible for resection at the time of diagnosis. About an additional 30% present with borderline resectable or locally advanced disease, some of whom may become eligible for curative surgery following chemotherapy. The remainder, which is more than half of all patients, are diagnosed at a stage where surgery is not possible.
When the tumor is caught at Stage I, when it is small and confined to the pancreas, the cure rate can reach 30 to 40% after surgery and adjuvant chemotherapy. By Stage IV, the disease is generally incurable. The tragedy of pancreatic cancer is not just that it is hard to treat, but by the time most people know they have it, the best treatment is already out of reach.
Why Immunotherapy Works — And Why Pancreatic Cancer Is Different
To understand the immunotherapy gap, it helps to understand what immunotherapy actually does.
The immune system is designed to detect and destroy abnormal cells, including cancer cells. But cancer is adaptable. Over time, tumors learn to evade immune detection by exploiting proteins called immune checkpoints, which are essentially biological signals that tell immune cells to stand down. Checkpoint inhibitor drugs block these signals, releasing the immune system’s brakes and allowing it to attack the tumor.
In melanoma, lung cancer, and several other cancers, this approach has been transformative. Cancer immunotherapy has shown remarkable effectiveness in the treatment of several solid tumors. These strategies consist of neutralizing antibodies against negative regulators of immune function, such as CTLA-4, PD-1, and PD-L1, impeding the ability of tumor cells to escape immune surveillance.
In pancreatic cancer, the same logic and the same drugs, have largely failed. Despite significant advances in immunotherapy in nearly all cancer types, progress for immunotherapy in pancreatic ductal adenocarcinoma has been difficult, particularly for immune checkpoint inhibitors. Though several clinical trials have evaluated these approaches, the results have been mostly disappointing, particularly compared to successes in other cancers.
The reason, researchers now understand, is that pancreatic cancer does not simply avoid the immune system. It actively defeats it.
Inside the Fortress: How Pancreatic Tumors Shut Down the Immune System
The scientific term for what surrounds a tumor is the tumor microenvironment, the complex ecosystem of cells, signals, and tissue that a cancer creates around itself. In most cancers where immunotherapy works, this environment is hostile to the tumor and friendly to immune cells. In pancreatic cancer, it is the opposite.
Pancreatic tumors actively reshape their immune environment by co-opting regulatory immune cells that normally shut down tumor-killing cells. In many pancreatic cancers, these regulatory cells overtake immune cells capable of killing tumors, effectively neutralizing immunotherapy before it can work.
The key culprits are cells called regulatory T cells, or Tregs. “Tregs are very suppressive immune cells,” said Dr. Katelyn Byrne, senior author of a landmark April 2026 study published in the journal Immunity and assistant professor at Oregon Health & Science University. “If there are a lot of them in a tumor, it’s extremely hard to get an anti-tumor immune response going.”
In plain terms: standard checkpoint inhibitors release the brakes on the immune system, but pancreatic tumors have already converted the immune system’s own soldiers into guards protecting the cancer. Releasing the brakes does not help if the drivers have switched sides.
A second barrier is physical. Pancreatic tumors are surrounded by dense, fibrous tissue called the stroma. This acts like a wall , blocking immune cells and drug molecules from physically penetrating the tumor, even when they have been activated. The immunosuppressive tumor microenvironment and low mutational burden are major barriers to the efficacy of immune checkpoint inhibitors in pancreatic cancer, a double obstacle that has frustrated a decade of clinical trials.
The Accountability Question: Why Did It Take This Long?
The biology is complex. But complexity alone does not fully explain the gap. Accountability requires asking harder questions about research investment, early detection, and institutional priorities.
Pancreatic cancer has historically received research funding that is disproportionately low relative to its death toll. The Pancreatic Cancer Action Network has consistently highlighted that pancreatic cancer research funding from the National Cancer Institute has lagged behind that allocated to cancers with significantly lower mortality rates.
There is also no approved early screening program for the general population, despite the fact that the survival data makes the case for early detection overwhelming. Screening programs for high-risk individuals report excellent survival outcomes, with rates ranging from 24% to 73% at five years. These results contrast drastically with the 13% five-year survival rate seen in patients diagnosed through standard clinical presentation.
The pharmaceutical industry’s incentive structure has also played a role. Pancreatic cancer’s rapid progression and complex biology make clinical trials expensive and slow, with high failure rates. For much of the past decade, investment has followed the path of least resistance, toward cancers where immunotherapy already showed early promise and where trial readouts were faster. Unfortunately pancreatic cancer offered neither.
This is beginning to change. But patients and families deserve to know that the gap was not inevitable, but in part, a consequence of where money and attention were directed.
Reasons for Cautious Hope: What Is Finally Working
The science published in 2025 and 2026 offers the most genuine grounds for optimism in years, not incremental improvements, but mechanistic breakthroughs that suggest researchers are finally attacking the right problems.
The OHSU Treg Breakthrough (April 2026)
The most significant recent development comes from Oregon Health & Science University. Researchers tested an experimental immunotherapy in mouse models known as agonistic CD40, which works differently from standard checkpoint inhibitors. Rather than targeting a single immune signal, the therapy broadly activates the immune response upstream. By reprogramming Tregs, the researchers were able to convert them from immune suppressors into cells that support anti-tumor activity.
This is a fundamental conceptual shift. Instead of simply releasing the immune system’s brakes, the treatment converts the tumor’s own defenses into attackers. “That’s what will allow us to move closer to durable, long-lasting immune responses for pancreatic cancer patients,” said Dr. Byrne.
The Elraglusib Survival Data
Adding the investigational drug elraglusib to standard first-line chemotherapy doubled 12-month overall survival from 22.3% to 44.4% in patients with metastatic pancreatic cancer. Median overall survival improved from 7.2 months with chemotherapy alone to 10.1 months with the combination therapy. For a disease where months matter enormously, this is a meaningful signal.
The First RAS Inhibitor
In early 2026, the Pancreatic Cancer Action Network highlighted the approval of the first RAS inhibitor to extend survival in previously treated metastatic pancreatic adenocarcinoma. This is a significant milestone given that KRAS mutations drive the majority of pancreatic cancers and have historically been considered undruggable.
Phase 3 Trials Beginning in 2026
In 2026, multiple Phase 3 trials are beginning for previously untreated metastatic pancreatic cancer to investigate whether adding targeted therapy to standard chemotherapy can improve patient outcomes. The field is moving from single-agent approaches to combination strategies that simultaneously activate the immune system and dismantle the tumor’s defensive architecture.
What Patients and Families Need to Know Right Now
For anyone facing a pancreatic cancer diagnosis or supporting someone who is, several practical points deserve emphasis.
Early detection remains the single most powerful factor in outcomes. Anyone with a family history of pancreatic cancer, or known genetic risk factors such as BRCA (Breast Cancer) mutations, should speak with their physician about monitoring and screening options. The survival data for screen-detected cancers is dramatically better.
Clinical trials are now a genuine option, not a last resort. The number of active trials has increased significantly, and several are now enrolling patients with earlier-stage disease. Asking an oncologist about trial eligibility at every stage of treatment is appropriate and important.
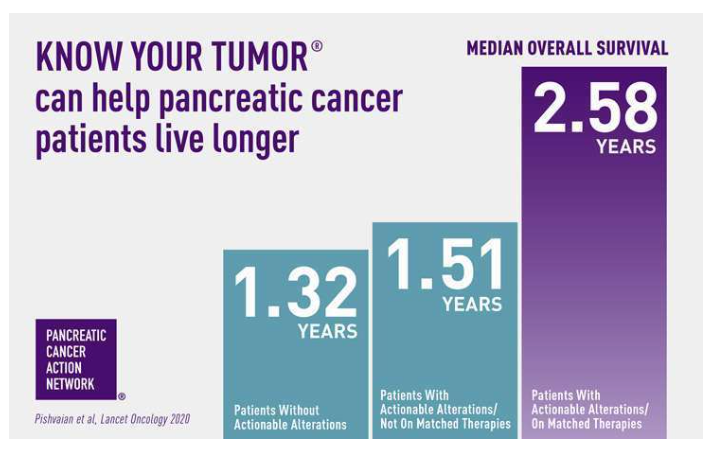
The Pancreatic Cancer Action Network offers free tumor profiling services through its Know Your Tumor program, matching patients to targeted therapies based on the specific genetic profile of their cancer. This is a direct, accessible resource that can open doors to treatments that would otherwise be missed.
Seeking a second opinion at a major cancer center with a dedicated pancreatic cancer program is always appropriate and can make a measurable difference.
Conclusion: The Science Is Finally Catching Up
For decades, pancreatic cancer has occupied a unique and terrible position in oncology: a disease where the tools that transformed every other cancer simply did not work, and where the reasons were only partially understood.
The OHSU research published in April 2026 represents something genuinely new. Not just a drug that performs slightly better, but a mechanistic understanding of why the immune system fails specifically in this disease and a concrete strategy to reverse that failure by reprogramming the tumor’s own defenses.
The immunotherapy gap is real. It was shaped by biology, by funding decisions, and by a decade of clinical disappointments. But for the first time in years, the research community has more than incremental progress to point to. The question now is whether the investment, the trials, and the institutional urgency will match the scale of the problem.
For the 52,740 Americans expected to die from pancreatic cancer in 2026, that urgency cannot come soon enough.
For support, resources, and information on clinical trials, visit the Pancreatic Cancer Action Network or call their free Patient Services line at 310-905-5169.


